Written by Evelyn Calado, MKin, CSCS, RKin

There is a persistent misconception that bone loss is something that “just happens” after menopause. By the time many women start thinking seriously about bone density, the process of loss is already well underway.
Osteopenia and strength training are directly linked, yet most women are not told how early bone loss actually begins.
Bone health is not a passive outcome of aging. It is an active, dynamic process shaped by hormones, mechanical loading, and energy availability across the entire female lifespan.
Understanding osteopenia requires understanding one central principle: bone is living tissue, constantly undergoing remodeling through the opposing actions of osteoblasts and osteoclasts.
Bone Remodeling: The Balance Between Formation and Breakdown
At any given moment, your skeleton is not static. It is metabolically active.
Osteoblasts are responsible for bone formation
Osteoclasts are responsible for bone resorption
In a healthy system, these processes are tightly coupled. Bone that is broken down is replaced with new, strong bone. The integrity of your skeleton depends on the balance between these two forces.
Estrogen plays a critical regulatory role in maintaining this equilibrium.
Estrogen as a Regulator of Bone Turnover
Estrogen is not just a reproductive hormone. It is deeply involved in musculoskeletal health.
It functions, in part, by:
Inhibiting excessive osteoclast activity
Supporting osteoblast survival and activity
When estrogen levels are stable, bone turnover remains balanced. But when estrogen becomes low or erratic, this regulatory system begins to fail.
Estrogen does not “leach calcium from bone.” Its decline removes inhibitory control over osteoclasts, allowing bone resorption to outpace formation.
The result is a gradual reduction in bone mineral density, what we clinically recognize as osteopenia, and eventually osteoporosis if left unchecked.
Perimenopause: The Underappreciated Inflection Point
Much of the conversation around bone health focuses on postmenopause. However, perimenopause is a critical and often overlooked phase.
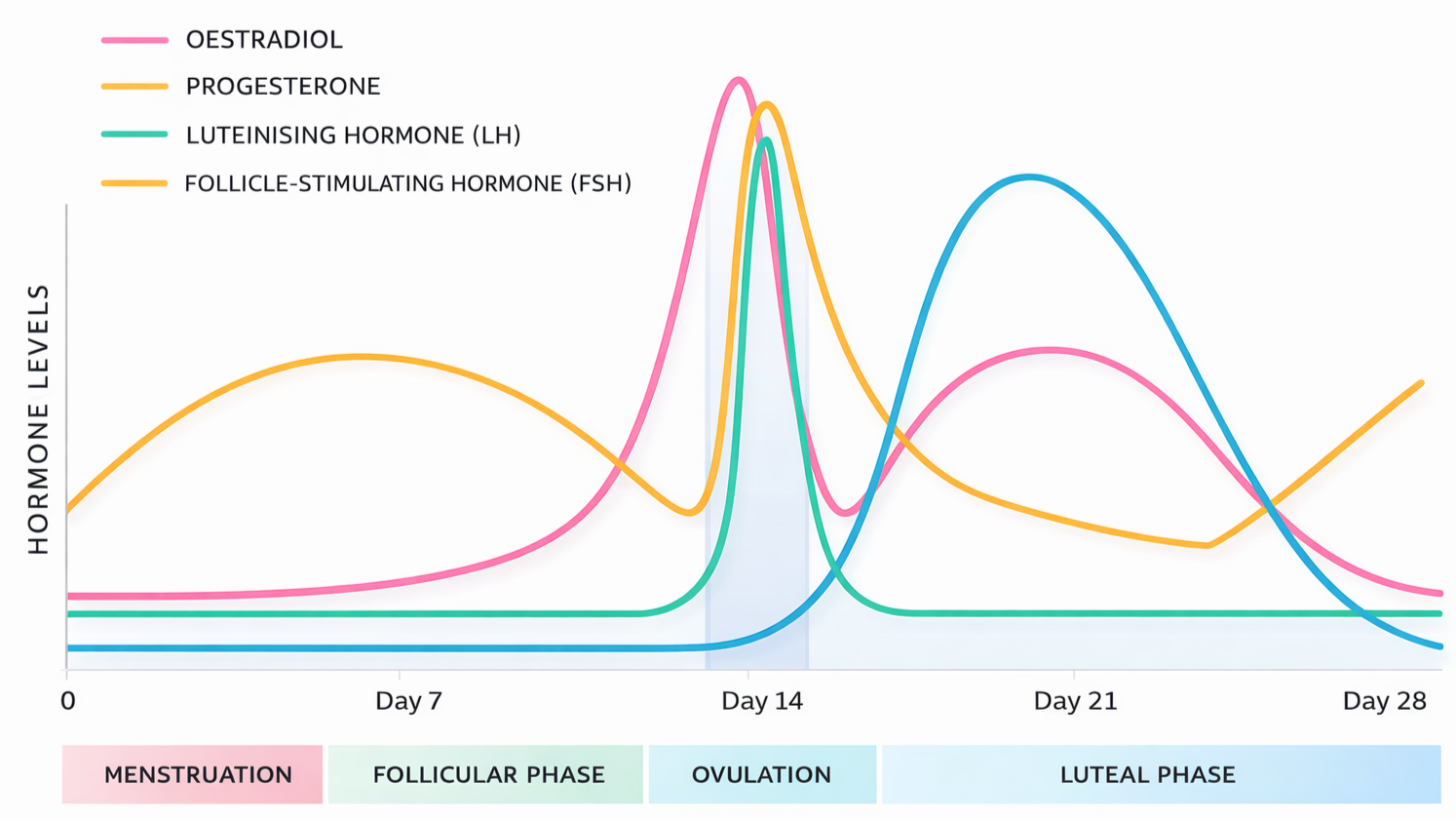
This is not simply a state of low estrogen. It is a state of hormonal volatility.
During perimenopause:
Estrogen levels fluctuate unpredictably
Progesterone exposure becomes inconsistent
The coordination of tissue remodeling processes becomes impaired
These fluctuations influence:
Bone turnover
Muscle protein synthesis
Recovery capacity
The net effect is a physiological environment that becomes increasingly catabolic, meaning tissue breakdown can begin to exceed tissue formation.
This is why bone density decline can begin before menopause is complete.
The Muscle–Bone Unit: Why Strength Matters
Bone does not exist in isolation. It is functionally linked to muscle through what is often referred to as the muscle–bone unit.
When muscle contracts, it exerts mechanical force on bone. This mechanical strain is the primary stimulus for bone adaptation.
Without sufficient loading, the body interprets bone as metabolically expensive and unnecessary, and osteoclastic activity increases accordingly.
Strength training directly targets this system.
Through high-load resistance exercise:
Muscle force increases
Mechanical strain on bone increases
Osteoblast activity is stimulated
Bone mineral density is preserved or improved
This is not a marginal effect. It is one of the most powerful non-pharmacological interventions available for maintaining skeletal integrity.
If you are unsure where to start, an individualized approach begins with an initial assessment.
Why Endurance Alone Is Not Enough
Many active women assume that being “fit” is sufficient to protect bone health. However, endurance training does not provide the same osteogenic stimulus as resistance training.
In fact, without adequate nutrition and strength work, high volumes of endurance exercise can:
Increase cortisol and systemic stress
Contribute to low energy availability
Impair bone formation
Bone health requires specific, targeted mechanical loading, not just general activity.
Why Strength Training Is Essential for Women’s Bone Health
Dr. Stacy Sims is explicit. Strength training is not optional for women. It is a lifelong requirement.
General recommendations include:
At least 2 to 3 strength sessions per week
Emphasis on heavy resistance, not just light weights
Inclusion of compound lifts and power-based movements
This becomes even more critical during perimenopause and beyond, when:
Muscle mass becomes harder to maintain
Hormonal support for tissue repair declines
The risk of accelerated bone loss increases
Strength training is not simply about preserving aesthetics or performance. It is about maintaining structural integrity.
For most people, this requires structure, progression, and accountability, which is exactly what personalized training provides.
The Compounding Effect of Muscle Loss
Muscle loss and bone loss are interconnected.
As muscle mass declines:
Mechanical loading on bone decreases
Bone formation signals weaken
Risk of fragility increases
Hormonal environments during this phase can also increase muscle protein breakdown, making it harder to maintain lean mass without intentional intervention.
This creates a feedback loop:
Less muscle leads to less bone stimulus, which leads to weaker bone and higher injury risk.
Strength training interrupts this cycle.
Bone Health Is Built, Not Preserved
One of the most important reframes is this:
You are not trying to hold on to bone. You are trying to continually build and reinforce it.
Bone is responsive tissue. It adapts to the signals it receives.
If the signal is inactivity, bone loss occurs
If the signal is chronic stress without adequate fuel, bone loss occurs
If the signal is heavy loading with adequate nutrition, bone strength improves
Perimenopause does not mark the end of this adaptability. It simply raises the stakes.
Final Thoughts
Osteopenia is not an inevitable consequence of aging. It is, in large part, the result of mismatched physiology, where hormonal changes are not met with appropriate mechanical and nutritional support.
Estrogen may set the stage, but behavior determines the outcome.
Strength training, done consistently and with sufficient intensity, provides the necessary stimulus to:
Maintain bone mineral density
Preserve lean muscle mass
Counteract the catabolic shifts of hormonal fluctuation
For women entering perimenopause, this is not optional. It is essential.
And the earlier this foundation is built, the more resilient the system becomes over time.
This is why most of the women we work with are already incorporating structured resistance training before these changes begin, many of them through our hybrid coaching program.
Source
Dr. Stacy Sims, ROAR