Written by Michael Crawley, BSc, BPT, CSCS
Nearly 100 years ago, Earnest Codman coined the term “frozen shoulder” and highlighted three clinical issues (Salamh et al. 2025):
Difficult to define
Difficult to treat
Difficult pathology to explain to patients
Those three points still hold true today.
Multiple structures and pathological findings have been implicated in the development of frozen shoulder. This includes the accumulation of immune system mediators, thickening of ligaments, and altered collagen translation (Pandey and Madi 2021). Clinically, this presents as a shoulder with reduced range of motion in both active and passive flexion, abduction, and external rotation (as seen in the image below).
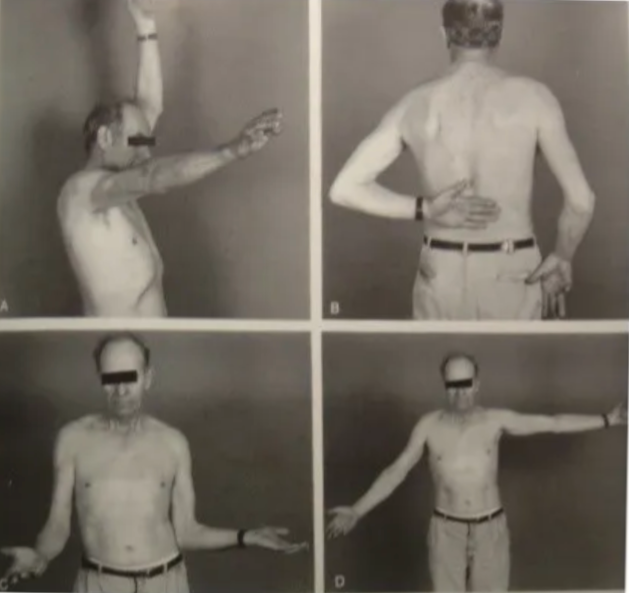
Figure 1: Reduced Shoulder range of motion (ROM) with frozen shoulder
The Real Impact of Frozen Shoulder
A scoping review examining how people experience and live with frozen shoulder demonstrates how debilitating and impactful the condition can be. King and Hebron (2023) identified five major themes:
“Dropping me to my knees, due to the pain”
Struggle for normality
Emotional change for self
Challenges through the healthcare journey
Coping & adapting
This highlights that frozen shoulder is not just a physical limitation. It can significantly alter how someone functions and experiences their daily life.
Unfortunately, frozen shoulder demonstrates a bias towards a particular demographic. Females in the 40–60 age category take the brunt of diagnoses. To rub salt in the wounds, females are more likely to experience a more prolonged and symptomatic course compared to male counterparts.
Types of Frozen Shoulder
Frozen shoulder can be broadly classified into two categories (Pandey and Madi 2021):
Primary:
A stiff shoulder developing with no known cause. However, there are commonly linked conditions, most notably diabetes mellitus and thyroid dysfunction. The incidence of frozen shoulder can reach as high as 30% in individuals with diabetes.
Secondary:
A stiff shoulder with an underlying cause such as direct trauma (e.g. a fall), infection, or inflammatory conditions.
The Three Stages of Frozen Shoulder
Frozen shoulder follows a series of stages, delineated by changing symptoms (Date and Rahman 2020). While approximate timelines are often attached, there is significant variability, and for some individuals, full resolution may not occur within 3–5 years.
Freezing Stage (Stage 1: 2–6 months)
Predominantly characterised by moderate to severe pain and partial restriction of ROM
Early stages may present with pain and only terminal loss of ROM
This stage can be confused with rotator cuff tendinopathy. However, ROM does not progressively worsen in tendinopathy, whereas it continues to worsen with each follow-up in frozen shoulder.
Frozen Stage (Stage 2: 4–12 months)
Characterised by both pain and stiffness in varying proportions
Early phase tends to be more pain-dominant
Later phase becomes more stiffness-dominant
Thawing Stage (Stage 3: 6–26 months)
Characterised by minimal pain
Gradual resolution of stiffness
Progressive return of movement
Pathologically, this reflects a gradual reduction in inflammation and restoration of movement.
Treatment and Management Across the Stages
What actually works, and when it matters
The research on the effectiveness of treatments for frozen shoulder remains conflicting. However, a conservative approach is typically recommended as the starting point (Date and Rahman 2020).
Common interventions include:
Analgesics
Physiotherapy
Intra-articular injections
Suprascapular nerve block
Early Stage: Movement Within Tolerance
In the early stage of frozen shoulder, gentle stretching and mobility exercises within a pain-free range are advised (Date and Rahman 2020).
Creativity can play a key role here, as Louis Gifford, the brilliant pain specialist, stresses. In his book Aches and Pains, he explains how adjusting body position can influence the amount of pain-free range available to a limb.
The videos below demonstrates this concept. The key idea is simple:
The arm can move relative to the body
Or the arm can stay fixed while the body moves around it
Shoulder Range of Motion Wall Drills:
https://youtu.be/9_GwO7r24hM
Passive and active-assisted exercises can also be incorporated. These reduce the working stress on affected structures, allowing the humerus to move through range without generating or exacerbating pain.
Active Assisted and Passive Shoulder:
https://youtu.be/072jZDVW-ac
As Pain Settles: Introducing Strength
As pain begins to reduce and become more manageable, strengthening exercises can be introduced.
Here, the principle that “the dose and position make the poison” becomes particularly relevant.
Using isometrics in varying positions and directions allows for global loading through the shoulder while staying within tolerable limits.
Entry Level Isometric:
https://youtu.be/mDzgyyKlzZo
Later Stages: What Are Mobilisations Actually Doing?
Mobilisations performed by a physiotherapist in the later stages have shown some utility. However, the mechanism behind their effectiveness is contested.
For many years, the prevailing thought was that inferior mobilisation directly impacted the shoulder joint capsule. However, Jeremy Lewis, a well-known Australian shoulder specialist, has pointed out that a physiotherapist would need to generate approximately 600kg of force to meaningfully affect the capsule.
I am not aware of many Canadians with a 600kg deadlift.
The best approach at this stage would be to continue to progress strength training through pain free range.
Injections and Medical Management: Timing Is Key
Outside of physiotherapy, injections and pharmacological treatments are often used.
Nonsteroidal anti-inflammatories have shown little impact in the case of frozen shoulder. Intra-articular steroid injections, however, have demonstrated positive effects, particularly when used at the right time.
Again, Jeremy Lewis stresses that these injections must be used in the early stages, when pain is highest. This reinforces the importance of early and accurate diagnosis.
A similar pattern is seen with suprascapular nerve blocks, which can also have a positive effect on pain relief when applied early (Date and Rahman 2020).
Surgical Options: Often Less Helpful Than Expected
Surgical options are available, but often yield little additional benefit.
Beard et al. (2018) found no clinically significant benefit of shoulder arthroscopy compared to sham surgery. This was further supported by the large UK FROST trial (Corbacho et al. 2021), which reported that early physiotherapy was more cost-effective and accessible compared to invasive and costly surgical approaches.
Interestingly, manipulation under anaesthetic, which previously had negative connotations, has shown some efficacy. This likely relates to the reduction of muscle guarding and tension that can develop with frozen shoulder. When under anaesthetic, this guarding effect is temporarily removed.
Looking Beyond the Shoulder
An important point that is often not expressed or evaluated in the research is that frozen shoulder may be a sign of broader health issues, stemming from multiple systems in the body.
In many cases, it can act as a wake-up call to incorporate strength and conditioning into your lifestyle and address other health metrics.
You may not be able to train the affected side in the same way, but there are still many full-body exercises that can be performed without exacerbating the shoulder:
Towing a sled
Belt squat
Walking lunges
Step-ups
Why This Matters
There are three key reasons why this approach is important:
Approximately 1 in 5 people go on to develop similar symptoms in the opposite shoulder (Pandey and Madi 2021)
Sedentary individuals are more likely to receive a frozen shoulder diagnosis
Well-designed strength and conditioning programs can positively influence the systems linked to frozen shoulder development, including endocrine, immune, and cardiovascular systems
Deeper Dive into Causation and Management
Recent research has continued to highlight the multi-faceted nature of frozen shoulder and the challenges associated with its management (Navarro-Ledesma 2025a).
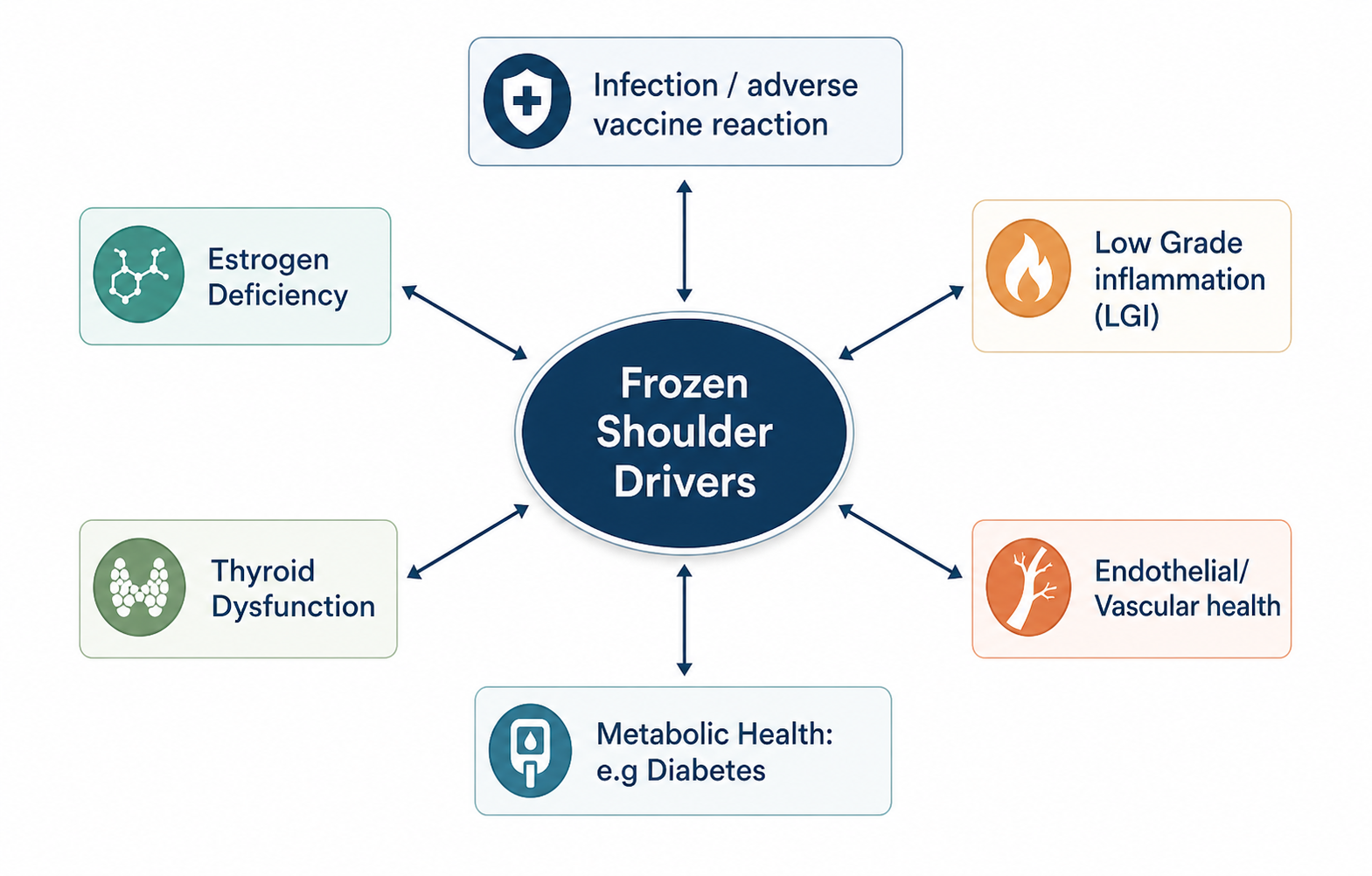
This is not a condition driven by a single structure or isolated tissue. Instead, it reflects the interaction of multiple systems within the body.
The diagram below highlights this well. Rather than being caused by one specific issue, frozen shoulder appears to sit at the intersection of several physiological systems, all of which can influence one another.
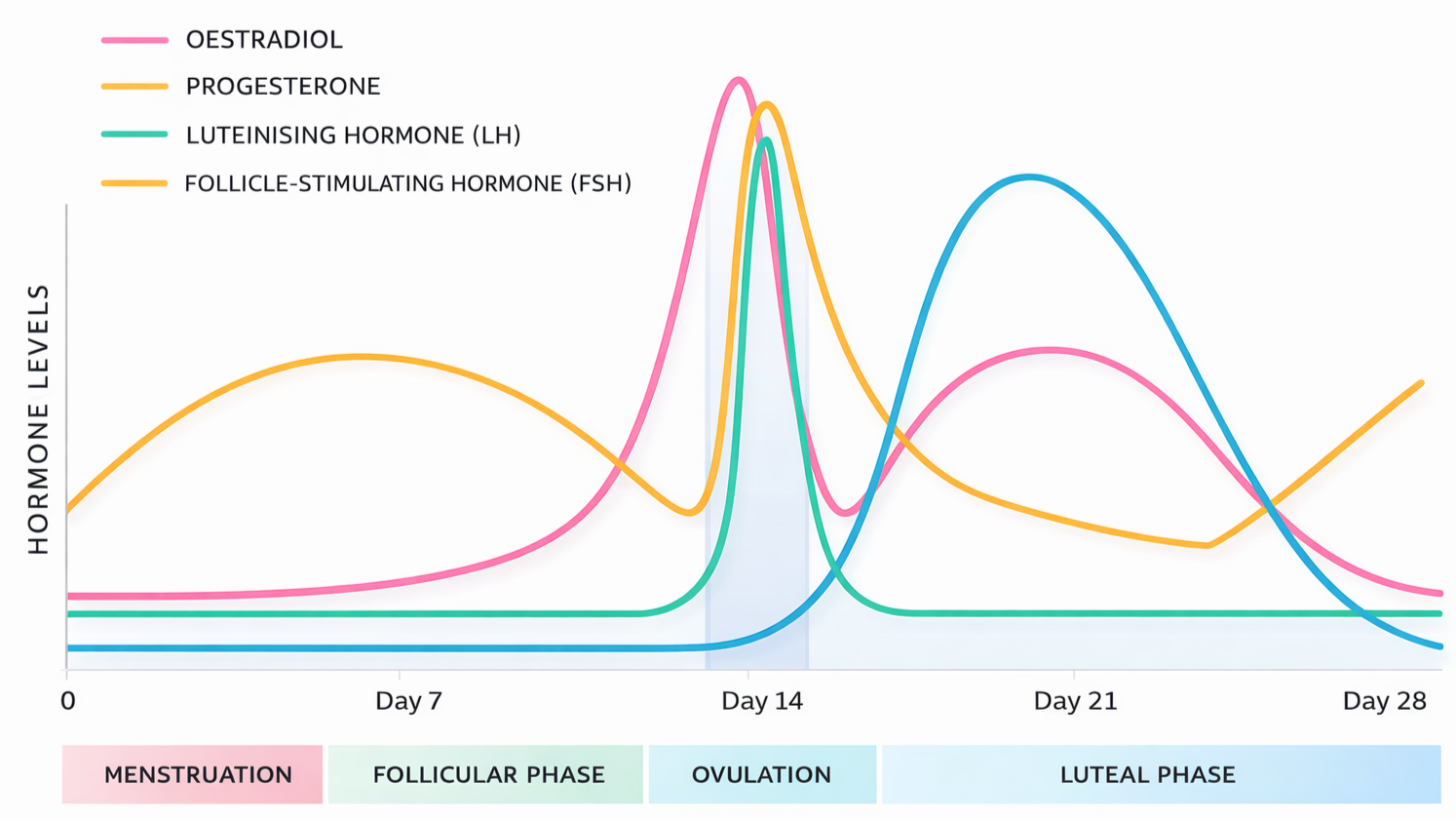
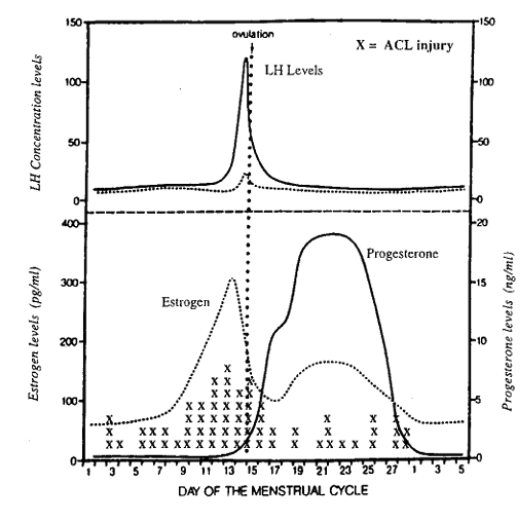
Estrogen and Menopause
One of the more consistent patterns seen in the research is the increased prevalence of frozen shoulder in peri-menopausal women. This has led to estrogen being identified as a key player in its development (Wend et al. 2012).
As shown in figure below, estrogen has effects that extend well beyond the reproductive system. Its influence spans multiple systems that are directly relevant to frozen shoulder.
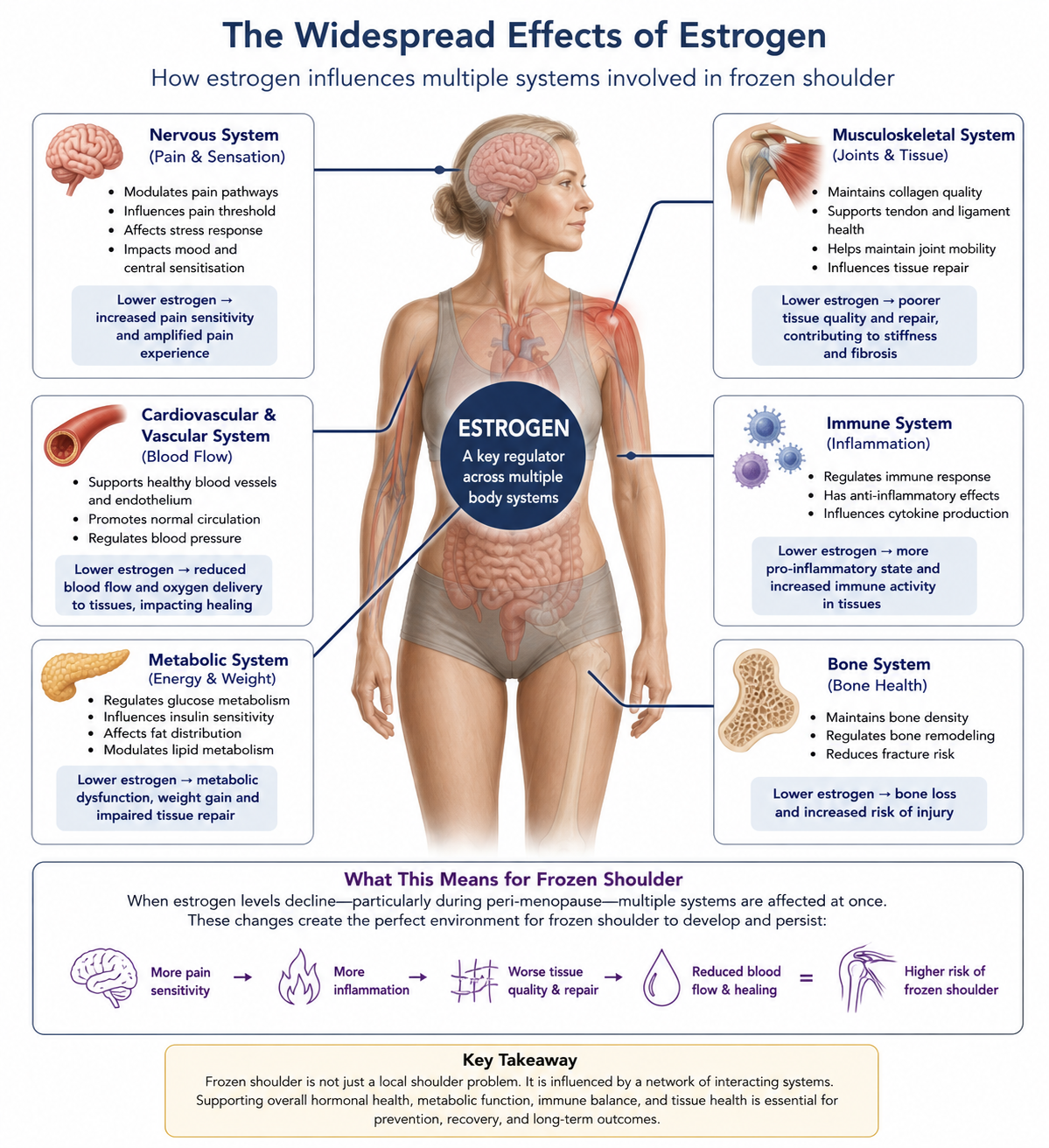
Neuroendocrine System
Declining estrogen levels can influence the nervous system through several mechanisms, impacting pain thresholds, resilience to stress, and central sensitisation.
A useful way to think about this is the “fire alarm” analogy.
You leave the bacon on the grill too long and the fire alarm goes off because of the smoke. There is no fire, but the system reacts as if there is.
With reduced estrogen levels, the threshold for triggering that “alarm” can become lower. The result is an amplified pain experience, even when the underlying tissue irritation may not fully justify it.
Metabolic System
Estrogen also plays a key role in fat metabolism, glucose regulation, and resistance to oxidative stress.
When these systems are disrupted, it can create an internal environment where tissue repair is compromised. This contributes to fibrosis, which is a hallmark of frozen shoulder.
Immune System
The same pattern continues within the immune system.
Declining estrogen levels tend to promote a more pro-inflammatory state. Immune system mediators accumulate within the tissues involved in frozen shoulder, and when combined with metabolic dysfunction, this can further drive the condition.
Targeting the System, Not Just the Shoulder
The research highlights how frozen shoulder is influenced by multiple systems, not just the shoulder itself. As a result, management is not limited to physiotherapy or surgical intervention alone.
There are a number of factors that could be explored here, but for the purpose of this piece, three of the more relevant and actionable areas will be discussed below.
Strength and Conditioning
Well-designed and properly implemented strength and conditioning programs have demonstrated positive impacts on estrogen levels, muscle mass, and fat mass in menopausal women (Razzak et al. 2019).
As mentioned previously, even with an impacted and painful shoulder, this does not mean avoiding training altogether or waiting for full resolution before doing anything.
The whole-body and multi-system benefits of strength training can influence long-term outcomes indirectly. While the shoulder itself may be limited, the broader physiological adaptations still matter.
Nutrition
Diet quality also plays a meaningful role.
A nutritional approach centred around higher-quality, minimally processed foods has been shown to impact symptom severity in individuals with frozen shoulder (Hamed-Hamed et al. 2026).
In practice, the decision to implement a structured strength training program often leads to improvements in other lifestyle behaviours, including dietary choices.
In the same way that hormonal, metabolic, and immune factors can drive the development of frozen shoulder, lifestyle decisions can push back against these drivers. This not only has the potential to improve current symptoms, but also to reduce the likelihood of future development.
Sleep and Circadian Rhythm
Circadian rhythm and sleep regulate inflammatory processes, hormonal release, and tissue repair (Navarro-Ledesma 2025a).
These are central to both general health and the development and recovery of frozen shoulder, as well as adaptation to strength training and exercise.
This is where the entanglement of systems becomes more apparent.
Bringing It Together
Sleep, exercise, and nutrition can be thought of as a three-legged stool. Each supports the others, and removing one weakens the entire system.
Addressing these factors will not provide an immediate solution to frozen shoulder. However, they can set the conditions for recovery and reduce the likelihood of recurrence, particularly when considering that approximately 20% of individuals will experience similar symptoms in the opposite shoulder.
Summary and Takeaways
Frozen shoulder is a systems issue, not just a joint problem
Frozen shoulder is not a local condition. It can have significant and long-term effects on both physical and psychological well-being.
In some cases, it can be so debilitating that it alters how an individual functions day to day. That may sound hyperbolic, but when revisiting the five themes outlined earlier, alongside the number of systems involved, it becomes more understandable.
Approaching treatment with a reductionist lens, relying solely on an injection or a home exercise program, is akin to using a hammer where a scalpel is required. This sentiment is supported in a recent review by Brindisino et al. (2026).
Effective management requires a more nuanced and personalised approach that considers the multiple drivers involved:
Hormonal (endocrine)
Immune system (autoimmune / inflammatory)
Strength, mobility, and capacity
Cardiovascular health
Pain psychology (sensitisation and emotional drivers)
Structural factors
Circadian rhythm and sleep
Key Takeaways
General strength training can still be completed and is beneficial with a frozen shoulder diagnosis
Surgical interventions are often unwarranted and do not demonstrate superior outcomes
Frozen shoulder is multi-factorial, and lifestyle factors such as exercise, nutrition, and sleep play a critical role in both management and risk reduction
References
Beard, D. J. et al. 2018. Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial. The Lancet 391(10118), pp. 329-338. doi: 10.1016/S0140-6736(17)32457-1
Brindisino, F. et al. 2026. Beyond the capsule: an integrated perspective on the wide world of frozen shoulder. A collaborative viewpoint. Pain Management, pp. 1-20. doi: 10.1080/17581869.2026.2636725
Corbacho, B. et al. 2021. Cost-effectiveness of surgical treatments compared with early structured physiotherapy in secondary care for adults with primary frozen shoulder : an economic evaluation of the UK FROST trial. Bone Jt Open 2(8), pp. 685-695. doi: 10.1302/2633-1462.28.Bjo-2021-0075.R1
Date, A. and Rahman, L. 2020. Frozen shoulder: overview of clinical presentation and review of the current evidence base for management strategies. Future Sci OA 6(10), p. Fso647. doi: 10.2144/fsoa-2020-0145
Hamed-Hamed, D. et al. 2026. Impact of nutritional profile on pain and functionality in patients with frozen shoulder: a cross-sectional observational study. Frontiers in Medicine Volume 13 - 2026, doi: 10.3389/fmed.2026.1785577
King, W. V. and Hebron, C. 2023. Frozen shoulder: living with uncertainty and being in “no-man’s land”. Physiotherapy Theory and Practice 39(5), pp. 979-993. doi: 10.1080/09593985.2022.2032512
Navarro-Ledesma, S. 2025a. Frozen Shoulder as a Systemic Immunometabolic Disorder: The Roles of Estrogen, Thyroid Dysfunction, Endothelial Health, Lifestyle, and Clinical Implications. J Clin Med 14(20), doi: 10.3390/jcm14207315
Navarro-Ledesma, S. 2025b. Frozen Shoulder as a Systemic Immunometabolic Disorder: The Roles of Estrogen, Thyroid Dysfunction, Endothelial Health, Lifestyle, and Clinical Implications. Journal of Clinical Medicine 14(20), p. 7315.
Pandey, V. and Madi, S. 2021. Clinical Guidelines in the Management of Frozen Shoulder: An Update! Indian J Orthop 55(2), pp. 299-309. doi: 10.1007/s43465-021-00351-3
Razzak, Z. A. et al. 2019. Effect of aerobic and anaerobic exercise on estrogen level, fat mass, and muscle mass among postmenopausal osteoporotic females. Int J Health Sci (Qassim) 13(4), pp. 10-16.
Salamh, P. et al. 2025. An international consensus on the etiology, risk factors, diagnosis and Management for individuals with Frozen Shoulder: a Delphi study. J Man Manip Ther 33(4), pp. 309-320. doi: 10.1080/10669817.2025.2470461
Wend, K. et al. 2012. Tissue-Specific Effects of Loss of Estrogen during Menopause and Aging. Frontiers in Endocrinology Volume 3 - 2012, doi: 10.3389/fendo.2012.00019